
Equitable allocation of a COVID-19 vaccine

By Nissa Shaffi, NCL Associate Director of Health Policy
As the world waits with bated breath for the release of a safe and effective COVID-19 vaccine, one concern that is paramount is the proper distribution of the vaccine. According to leaders of Operation Warp Speed (OWS)—a coordinated partnership between the Department of Health and Human Services (HHS) and the Department of Defense (DoD)—detailed planning is ongoing to realize OWS’s lofty goal of delivering 300 million doses of a COVID-19 vaccine, with the initial doses available by January 2021.
Implementing a vaccine program of this magnitude is contingent upon precise coordination that traverses federal, state, local, tribal, and territorial governments. The prodigious task ahead is determining who would get the first initial doses of the vaccine upon release. The pandemic has further illustrated that communities most vulnerable to COVID-19 are often rife with systemic racism and socioeconomic factors conducive to higher infection rates. An initial limited supply of a vaccine will only intensify these inequities.
Multiple analyses conducted on the federal, state, and local levels confirm that people of color have experienced a *disproportionate burden of COVID-19 cases and deaths. Hispanic or Latinx, and American Indian and Alaskan Native (AI/AN) communities have experienced three times the rate of infection, and Black communities two times the rate of infection, compared to White populations. The CDC warns that this imbalance in morbidity and mortality is begotten by deep-seated disparities that stem from generations of racism and unaddressed social determinants of health.
To mitigate these inequities, the National Academies of Science, Engineering, and Medicine (NASEM) have formed a committee to establish an overarching framework addressing key considerations for the equitable allocation of a COVID-19 vaccine, including at-risk communities, priority populations, geographic distribution, scalable measures, and vaccine hesitancy.
The framework proposes four phases of vaccine distribution and their corresponding priority populations, as follows:
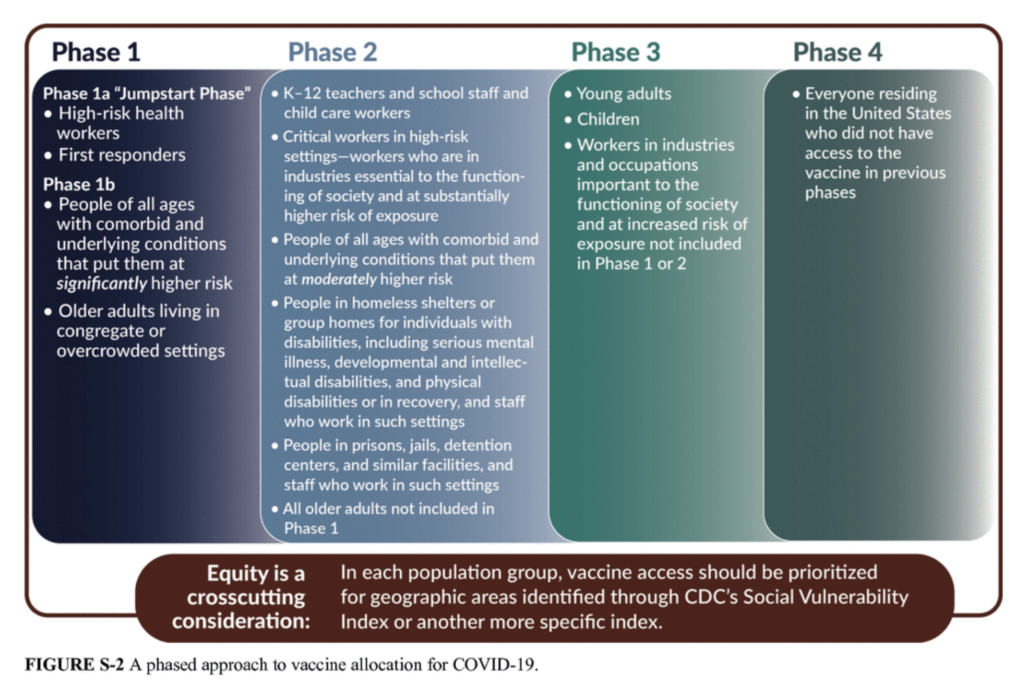
[Source: NASEM]
The above proposal will inform CDC’s Advisory Committee on Immunization Practices’ (ACIP) recommendations in advance of a COVID-19 vaccine release; and it was developed through careful consideration of CDC’s Social Vulnerability Index (CDC *SVI), and the apropos, COVID-19 Community Vulnerability Index (CCVI). To elucidate, these phases were designed with people of color in mind, as they experience heightened risk of exposure working in essential roles in society, and therefore succumb to higher rates of infection.
Another key component of the vaccine plan is addressing vaccine hesitancy. People of Color are significantly underrepresented in clinical trials and undertreated in medical settings. This phenomenon, compounded by a general mistrust of medical establishments by minorities, will prove to be a challenge when encouraging vaccine uptake. Community engagement will be essential in building trust among the vaccine hesitant and messaging should be delivered by community leaders, or healthcare providers that resemble the population they treat. Culturally competent care has proven to have favorable effects on health outcomes and it is critical in encouraging vaccine confidence.
Once a vaccine becomes available, health officials across the country will need to deploy resources and personnel to ensure access to the vaccine among our most vulnerable. As affirmed by U.S. Army Lt. Gen. Paul Ostrowski (OWS), “We have to be able to go beyond the pharmacies, the hospitals and so forth to get after nursing homes; to get after meatpacking facilities; to get after those that are sheltered [at home]. We have to get this out to all four corners of this nation.” Getting to a vaccine is a challenge in itself, but once its released, it’s all hands-on deck.
*Links are no longer active as the original sources have removed the content, sometimes due to federal website changes or restructurings












